

Motion Analysis, Multi-Omics, Novel Biosensors for Osteoarthritis Diagnosis and New Therapeutics Delivery
…………………………….
Musculoskeletal (MSK) Conditions
On 20 November 2024, the World Health Organization (WHO) dispatched an opportunity for the global health system addressing the importance of musculoskeletal (MSK) conditions (https://www.who.int/news-room/events/detail/2024/11/20/default-calendar/addressing-musculoskeletal-conditions–an-opportunity-for-health-systems-globally ). Key facts (https://www.who.int/news-room/fact-sheets/detail/musculoskeletal-conditions ) of MSK health indicates that they limit mobility, lower levels of well-being and reduce the ability to participate in society. The number of people living with MSK conditions is rapidly increasing due to population growth and ageing. MSK conditions include joints (arthritis), bones (osteopenia-osteoporosis) and skeletal muscles (sarcopenia). The United Nations (UN) established a platform for the decade for healthy aging 2021-2030 (https://www.decadeofhealthyageing.org/ ).
…………………………….
Why Osteoarthritis (OA)?
There are currently symptomatic therapies for OA and no efficient cure to the disease.
…………………………….
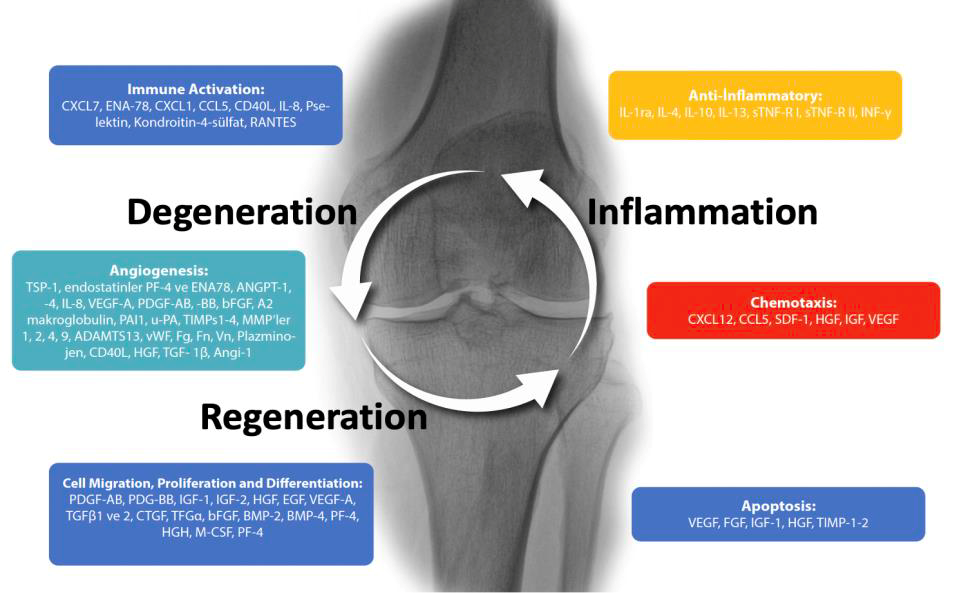
Figure 1. The intervening cascade of inflammation, degeneration and regeneration in osteoarthritis.
…………………………….
Osteoarthritis (OA) is the most common form of arthritis. It effects 15% of the global population over the age of 30 (GBD 2021 Osteoarthritis Collaborators. Global, regional, and national burden of osteoarthritis, 1990–2020 and projections to 2050: a systematic analysis
for the Global Burden of Disease Study 2021. Lancet Rheumatol 2023;5: e508–22). As a noncommunicable disease, it is a heterogeneous (1) and complex (2) disorder and/or condition with a cascade of intervening periods of inflammation, degeneration and regeneration in and around articular joints (Figure 1). It is presented by high rates of disability, comorbidity and mortality (3,4,5,6,7). The cardiovascular mortality rate is higher in Korean knee OA patients due to limited mobility (Oh M, Kim MY, So MW, Lim DH, Choi SJ, Lee JH, Her M, Kim SH, Lee S. Association between knee osteoarthritis and mortality: a serial propensity score-matched cohort study. Korean J Intern Med. 2023 Nov;38(6):923-933. doi: 10.3904/kjim.2023.222. Epub 2023 Nov 1. PMID: 37939669; PMCID: PMC10636544.). Only a few applications and therapeutics can currently decrease OA symptoms and cure is seldom observed as the disease progresses with regression. Most clinical outcomes such as decrease in pain and increase in function are usually recorded by semi-quantitative questionnaires. There is therefore an obvious need for the quantification of regeneration, if any, in OA related joint damage after therapies. The average time to physiotherapy and/or joint replacement surgery in most European and associated countries is furthermore about four to six months after decision. In some countries the duration may even go up to two years. Ten to twenty percent of the patients do still complain of pain after joint replacement surgery (https://osteoarthritisineurope.eiu.com/).
…………………………….
Not All Osteoarthritis Patients are the Same.
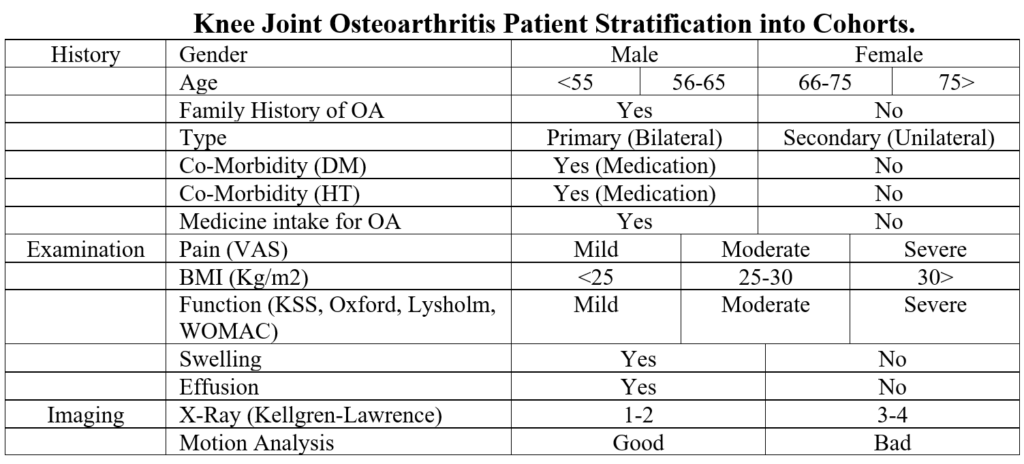
Research to determine subtypes of OA is currently carried out in various research centers (Ma j, Zhang K, Ma X, Wang H, Ma C, Zhang Y, Liu R. Clinical phenotypes of comorbidities in end-stage knee osteoarthritis: a cluster analysis. BMC Muskuloskeletal Disorders 2024;25:299.). A recent study identified 4 sub-types according to multi-omics of a hundred patients synovial sample analysis (Liu X, Lv Z, Shi D. Multi-omics analysis of synovial fluid identifies four distinct subtypes of osteoarthritis. Osteoarthritis & Cartilage 2024;32 (S): 1S467.) There are genomic, transcriptomic, proteomic, metabolomic and lipidomic pheno- and-endo-types that can present different molecular clinical and therapeutic sub-types of OA (Figure 2). Their pain, deformity and motion can also be different due to their age, sex, severity of their disease, obesity and co-morbidities (Table 1). In plain words, there are various types of conditions determined under the general name of this multi-genic and acquired wear and tear disease (Figure 2).
……………..
Table 1. Common characteristics of OA
| A cyclical disease with multiple phenotypes, multiple etiologies, heterogeneous and low inflammatory. |
| Advanced age, female gender, black race, heredity, increased body mass index, trauma, inactivity. |
| Morbidity and mortality. |
| Meniscus tear, intra-articular or periarticular fracture and ligament injury or joint dislocation in secondary OA. |
| The symptoms are cyclically progressing pain, swelling, limitation of movement and deformity. |
| Decrease in the thickness of the articular cartilage, deterioration of its molecular structure and change in its microarchitecture: change in chondroitin-keratan sulfate ratios: chondro-senescence. |
| Degeneration (catabolic degradation) through the cycle of fibrillation, destruction and regeneration (anabolic construction) in articular joint cartilage. |
| Thinning and sclerosis on the articular surface. |
| Subchondral cyst formation and painful osteophytes with inflammation in the subchondral bone. |
| Thickening of the joint capsule, synovitis and decrease in joint fluid: changes in metabolites. |
| Meniscus degeneration and displacement from the joint space. |
| Skeletal muscle atrophy: sarcopenia. |
| Wearing of tendons and ligaments: deterioration of balance due to laxity and increased risk of falling. |
…………………
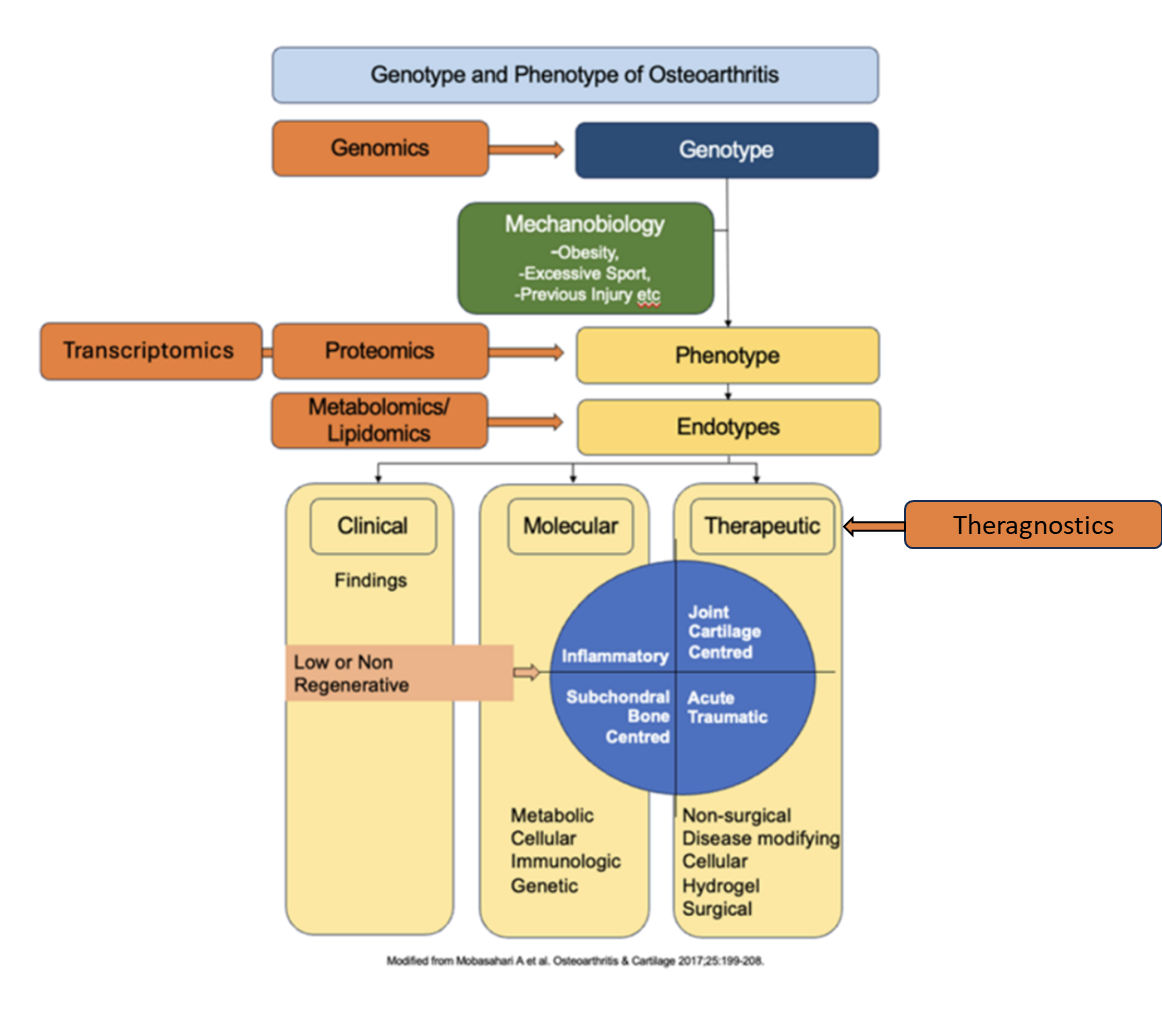
Figure 2. Geno-, Pheno- and Endo-Types of Osteoarthritis.
……………..
…………………..
How can we improve Osteoarthritis diagnosis and response to treatment?
Clinical practice relies on the history of the patient, physical examination and X-ray imaging mostly. Semi-quantitative questionnaires on pain and function may predict the natural course of the disease and response to treatment to some extent. Magnetic resonance is highly costly and the patient has to go to a medical center for imaging. Motion analysis, multi-omics and valid biosensors for the diagnosis and response to OA treatment are in their early phase of experimentation. Artificial intelligence-based motion analysis and multi-omics evaluations together with novel biosensor development for the diagnosis and response to treatment establish the core of this project proposal. Information derived from the multi-omics studies can be used for the development of new biosensors. Biosensors can then be used for the early diagnosis and response to treatment. New therapeutic outcomes and their sub-cutaneous delivery can be monitored by using these sensors.
What should be the decent treatment for Osteoarthritis?
Due to the multi-face of OA, there is not a single and the best method of treatment. Each individual patient needs special care and personalized treatment algorithms. Treatment modalities can be generalized as symptomatic and regenerative (Figure 3).
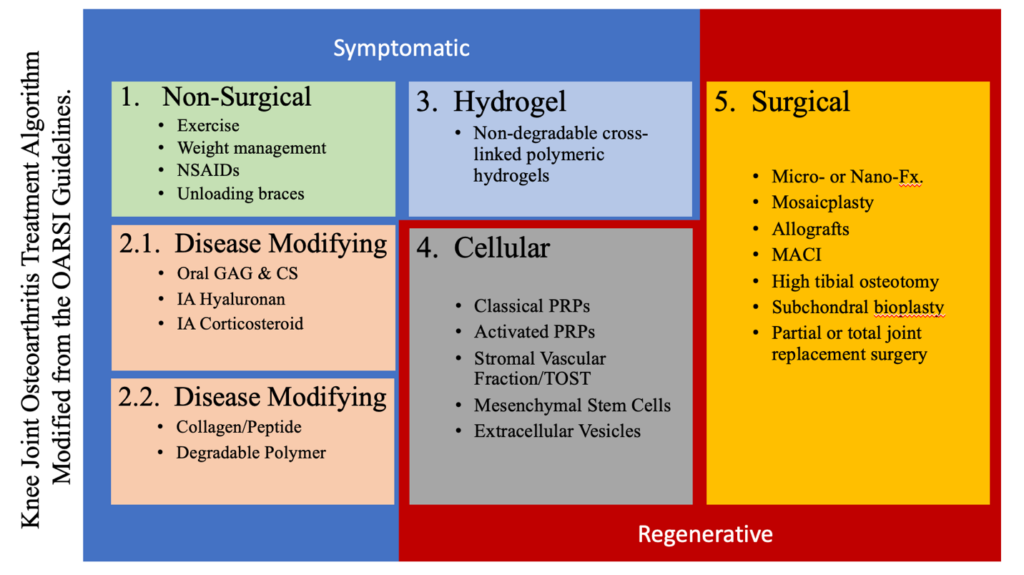
Figure 3. Current treatment algorithms for osteoarthritis treatment.
………………